Barriers and facilitators to women’s access to sexual and reproductive health services in rural Australia: a systematic review | BMC Health Services Research
The search retrieved 1,024 unique records that were screened for inclusion based on their title and abstract with 50 articles meeting the inclusion criteria. Reasons for exclusion at the full-text phase are described in the PRISMA diagram (Fig. 2).
Fig. 2
PRISMA flow diagram of screening process
Characteristics of selected studies
The characteristics of the 50 included studies are presented in Table 3. Most studies analysed women’s access to primary care services (n = 29; 58%), followed by hospital services (n = 14; 28%), health promotion and prevention (n = 5; 10%), and specialist care (n = 2; 4%). Over half (n = 28) of the studies examined barriers and facilitators from the women’s perspective, just under half (n = 25) were from the provider or clinician’s perspective, and four examined barriers and facilitators from both perspectives. Of the 50 studies, most studies employed a qualitative approach to data collection (n = 33; 66%), followed by quantitative (n = 11;22%), and mixed-methods (n = 6; 12%).
Table 3 Summary table of included articles (n = 50)
The highest proportion of studies were conducted in New South Wales (NSW) (n = 14; 23%), followed by Victoria (VIC) (n = 13; 22%). The geographic classifications used to define rurality or remoteness areas varied across the studies, including the ASGS-RA (n = 10), Australian Statistical Geography Classification Remoteness Areas (ASGC-RA) (n = 3), Accessibility/Remoteness Index of Australia (ARIA, ARIA+) (n = 3), and MMM (n = 1) (Supplementary File 4). Thirty-three studies did not use a geographic classification to define the location.
Service setting
The highest proportion of studies were focused on maternity care settings (n = 21; 42%), followed by abortion services (n = 11; 22%), screening and testing (e.g., STI, cervical, breast screening) (n = 8; 16%), other women’s health services (n = 6; 12%), and family planning (n = 4; 8%). Other women’s health services encompassed gynaecology, sexual healthcare, reproductive services, and experience accessing a community-based women’s health clinic. Studies investigating access to maternity care focused on various aspects of care, including antenatal and postnatal services in regional, rural, and remote Australia. Six studies were focused on Aboriginal and Torres Strait Islander women’s experience of maternity care. Studies examining access to abortion services were primarily focused on rural and regional access to medical termination of pregnancy (MToP) (n = 8), as opposed to surgical termination of pregnancy (SToP) (n = 2), and one study examined both. Studies that focused on screening and testing included sexually transmissible infections (STI) (n = 4), cervical screening programs (n = 3), including self-sampling (n = 2), and breast cancer screening (n = 1). Family planning predominantly focused on rural and regional women’s experiences of unintended pregnancy and accessing family planning services, such as options counselling, emergency contraception, abortion services, or antenatal care.
Barriers and facilitators
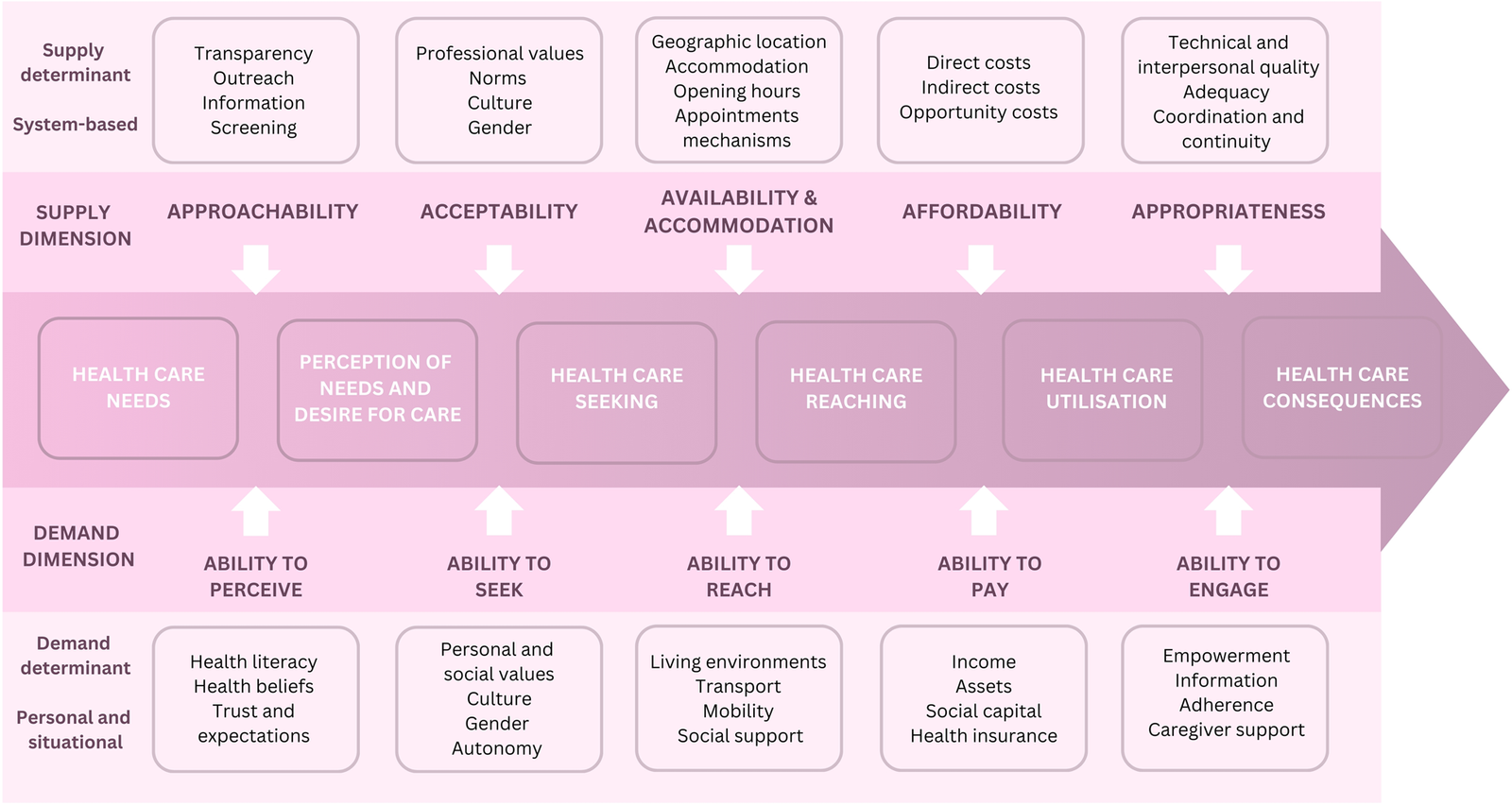
Key barriers and facilitators are presented under the five dimensions of the patient-centred access to healthcare model (Fig. 1) [12]. Barriers and facilitators are presented for both the supply and demand dimensions of the model, including approachability (ability to perceive), acceptability (ability to seek), availability and accommodation (ability to reach), affordability (ability to pay), and appropriateness (ability to engage). It is important to note that some of the supply and demand factors complement each other.
Approachability and ability to perceive
Approachability represents the capacity of a health system to provide services so that women with health needs can identify and reach them [12]. Health services can make themselves known to women from different social, cultural, or geographical groups through transparency, providing information (e.g., about available treatments), and outreach activities. Individual factors such as health literacy, knowledge and beliefs about health determine the ability to perceive healthcare needs. The dimensions of approachability and ability to perceive were explored in 28 studies across primary care (n = 10), hospital (n = 10), and health promotion and prevention (n = 8) settings.
Supply barriers
Three main barriers were identified for approachability: insufficient information, fragmented healthcare pathways, and limited internet access. Insufficient information primarily related to gaps in the information provided by GPs around maternity care providers [38] and abortion options [15, 39]. Another study reported that women lacked information on available local services and support [40]. Studies reported gaps in provider knowledge and awareness around abortion, contributing to insufficient information [41,42,43,44]. Fragmented healthcare pathways were noted in two studies [45, 46], particularly concerning access to local maternity care providers and options for unintended pregnancy. Under the dimension of approachability, fragmented pathways refer to the lack of transparency and visibility of services, making it difficult for women to identify and access the care they need. The healthcare pathways for unintended pregnancy were described as unclear and disjointed compared to those for antenatal care [45]. Providers also noted the lack of referral pathways, particularly to post-natal care [47]. Limited internet access was described as a barrier inhibiting individuals from obtaining information about various healthcare services, contributing to restricted awareness and choice of providers [48].
Demand barriers
Three main barriers emerged related to women’s ability to perceive healthcare: low health literacy, limited awareness, and difficulties in navigating the health system. The barrier of low health literacy was predominantly related to cervical screening [49] and STI symptoms, testing, and treatment [50]. Limited awareness was identified for available information regarding local and financial support, such as the Patient Assisted Travel Scheme (PATS) for those required to relocate [46]. Difficulties in navigating the health system and coordinating services were reported in studies focused on unintended pregnancy [45] and maternity care [46]. For example, women reported difficulties in locating appropriate services, often relying on word of mouth or personal contacts to identify services [45].
Supply facilitators
Two main facilitators were identified for approachability: health system improvements and enhanced education and institutional approaches. Health system improvements pertained to changes to the health system, such as providing culturally accessible information and roles for Aboriginal Health Practitioners (AHP) to work with the community and coordinate access to screening services [51]. Additional improvements included direct referrals from GPs to services [52] and utilising midwifery group practice models for more efficient health system navigation for antenatal care [53]. The second facilitator was enhanced education and institutional approaches. This encompassed recommendations for comprehensive, culturally respectful, and accessible information about puberty and menstruation within the school health curriculum [54]. One study [55] suggested using a whole-of-institutional approach in healthcare settings (similar to whole-school approaches) to support change at multiple levels, and shifting institutional culture around abortion through de-stigmatising policies and protocols. Finally, improved dissemination of information regarding available relocation subsidies was recognised as a facilitator to alleviate the financial burden on women relocating for maternity care [46].
Demand facilitators
Three facilitators were identified for women’s ability to perceive healthcare: information access, knowledge and awareness, and culturally appropriate information. Information access was primarily related to internet access, as this was the most common way women accessed information, and ease of access to information determined the choice of provider [48]. Knowledge and awareness were key themes in several studies, predominantly focusing on awareness of services [56] and enhancing knowledge about symptoms and testing of STIs [50]. The final facilitator related to the ability to perceive was culturally appropriate information, such as suitable health promotional material for Aboriginal and Torres Strait Islander women and culturally inclusive education sessions for antenatal care [51, 57, 58].
Acceptability and ability to seek
Acceptability relates to cultural and social factors that affect a woman’s ability to accept or seek health services or aspects of them. For example, the gender or social group of the provider or the beliefs associated with systems of medicine may reduce the acceptability of seeking care [12]. The ability to seek care is related to the concepts of autonomy and the capacity to choose to seek care, knowledge about healthcare options, and individual rights that determine the intention to obtain healthcare. The dimensions of acceptability and ability to seek were explored in 30 studies across primary care (n = 15), hospital (n = 10), and health promotion and prevention (n = 5) settings.
Supply barriers
Three primary barriers were identified for acceptability: negative provider attitudes, low-quality care, and privacy concerns. Negative provider attitudes were frequently reported by women and included GPs’ unwillingness to refer for abortion services or denying care altogether, leaving women needing to locate willing providers themselves [15, 39, 52, 55, 59]. Provider resistance, stigma and religious objections were reported in studies focused on abortion or family planning services [41, 59, 60]. Additionally, negative provider attitudes were reported across studies providing other health services, including STI testing [50] and maternity care for Aboriginal women [61]. Low-quality care was a reported barrier in studies of abortion services, specifically the impact of abortion stigma on the quality of care in the context of healthcare interactions [55]. Privacy concerns were identified across multiple studies, including family planning [59], abortion services [15], and STI testing [62].
Demand barriers
Three barriers were identified for women’s ability to seek healthcare: lack of cultural safety, stigma, embarrassment and perceived judgment, and community context challenges. Lack of cultural safety primarily affected maternity care for Aboriginal and Torres Strait Islander women, whereby standard maternity care was not deemed culturally safe, with limited cross-cultural understanding of medical care [63]. The absence of inclusive services was a barrier to sexual health services [64]. Stigma, embarrassment, and perceived judgment from health professionals were barriers highlighted in a study involving young women regarding STI testing [50]. Community context challenges related to the inherent challenges of living in a small rural community [45, 59]. Some studies reported barriers, such as fear of stigmatisation and the lack of confidentiality in a small town, rural culture, and community ties [45], as well as limited local resources resulting in a lack of agency [46].
Supply facilitators
Three facilitators were identified for acceptability: inclusive and culturally sensitive practices, enhanced privacy with flexible service delivery, and improved health system practices. Culturally sensitive practices involved ensuring cultural safety and consulting women on their cultural needs around birth [63]. Inclusive practices identified in studies related to communication, the use of gender-neutral language, and the incorporation of visual signs of an inclusive environment [64]. Several facilitators pertaining to enhanced privacy with flexible service delivery were observed, including self-sampling for cervical screening tests and telehealth for MToP appointments [15, 65]. Self-cervical screening not only increased privacy but also empowered Aboriginal women to be in charge of women’s business [65]. Improved health system practices related to services, such as normalising family planning within the health system, including the right to make reproductive decisions regarding if, how and when to have children [59]. Additionally, the provision of high-quality abortion care with active assistance from healthcare providers in accessing such care [55].
Demand facilitators
The main facilitator for women’s ability to seek healthcare was related to care preferences. Birthing in the local community was reported to be a positive experience for women [66]. Services that offered greater discretion and privacy were reported as facilitators in several studies, particularly in rural areas [15, 48]. The preference for communication style regarding care was also noted as a facilitator [56, 67]. For example, some studies found that text messaging assisted in managing appointments and providing pertinent information to patients, particularly for younger age groups. Conversely, older patients were perceived to prefer receiving a letter in the post [56, 67].
Availability and accommodation and ability to reach
Availability and accommodation refer to the ability to access health services and healthcare providers, both physically and promptly. Availability means enough health resources to provide services, including the providers’ characteristics (e.g., presence of the health professional, qualification) and how services are delivered [12]. Factors such as a woman’s mobility, transportation access, employment flexibility, and knowledge about health services determine the ability to reach healthcare. The dimensions of availability and accommodation and ability to reach were examined in 38 studies across hospital (n = 19), primary care (n = 10), health promotion and prevention (n = 6), and specialist care (n = 3) settings.
Supply barriers
Three barriers were identified for availability and accommodation: poor local access, inadequate health service availability, and limited provider availability. Poor local access was related to the lack of and fragmented local services. For example, ultrasound or pathology services were not available at the same location as the care provider, requiring patients to travel [58, 61, 68]. Limited local aftercare and support were identified as a barrier to postnatal care [69, 70]. For instance, women who travel to another location to give birth were limited in local postnatal support once returning [69, 70]. Inadequate health service availability was attributed to women’s difficulty in obtaining appointments due to limited availability or long wait times [48, 52, 59, 66, 70, 71]. Women also reported delays in care or procedures due to long wait times for pre-appointment screenings, such as blood tests or ultrasounds [39, 48, 59]. Limited provider availability was particularly noted for female doctors, rural GPs, and AHPs [21, 59, 61, 70]. Studies also reported a lack of available providers for MToP appointments [70], pharmacists dispensing mifepristone and misoprostol [41], and a low number of rural practitioners willing to provide abortion or obstetric services [45]. Rural workforce challenges were a prominent barrier reported by providers [57, 58, 72,73,74]. Recruitment and retention of midwives, obstetricians, GP obstetricians, and paediatricians was reported to be one of the biggest threats to the sustainability of rural maternity services [73,74,75].
Demand barriers
Three barriers were identified that impacted a woman’s ability to reach healthcare: transportation issues, increased travel, and relocation for care. Transportation issues were particularly relevant for women without a driving licence or car, as they had to depend on public transportation or family and friends [67]. Increased travel was a commonly reported barrier across most studies, including long distances to access services [21, 39, 61, 66, 69, 71], travel-related inconveniences [40], and the distance to culturally appropriate care [51]. For example, one study [61] reported that Aboriginal women in remote communities had to travel long distances, including night-time travel by public bus for antenatal appointments, with only one available return bus service per day. Relocation for care was predominantly reported in studies focused on maternity care for Aboriginal and Torres Strait Islander women [61, 63].
Supply facilitators
Facilitators identified for availability and accommodation encompassed the enhancement of local service provision and capacity, and increased resource accessibility. Strategies to enhance local service provision and capacity involved increasing their capacity [21], optimising the use of shared maternity care and telehealth [46], MToP telehealth availability [15], and on-site ultrasound services [48]. Additional facilitators related to new services, such as reopening local services [46], rural birthing services [66], early postnatal supports [66], and an increased number of pharmacies stocking mifepristone and misoprostol [60]. Local access to an Indigenous midwife or AHP, as well as the provision of maternity home visits for Aboriginal communities was also identified [61, 63]. Finally, increased resource accessibility predominantly centred on menstrual health and access to sanitary products. Facilitators included providing free and discreet sanitary products and waste disposal facilities, availability of washing amenities and pain management in schools, and improving the availability of environmentally friendly, reusable products in rural locations [54].
Demand facilitators
One facilitator was identified for women’s ability to reach healthcare: time and travel efficiency. This was related to telehealth appointments [76] and human papillomavirus (HPV) self-screening [65], which reduced travel requirements and saved time.
Affordability and ability to pay
Affordability pertains to a woman’s economic ability to allocate resources and time to necessary health services. The direct costs of services, related expenses, and the potential loss of income influence it. Affordability can differ based on the type of service and relies on the ability to acquire the resources needed to cover care costs [12]. The ability to pay describes the capacity to generate economic resources through income for healthcare services without suffering catastrophic financial consequences, such as selling a home. Factors such as poverty, social isolation, or debt can restrict a woman’s ability to pay for necessary care. The dimensions of affordability and ability to pay were explored in 26 studies across hospital (n = 10), primary care (n = 7), health promotion and prevention (n = 6), and specialist care (n = 3) settings.
Supply barriers
Two primary barriers to affordability were identified: high direct costs and costs associated with essential products. The high direct costs identified across multiple studies included limited bulk-billing options [50, 56], the cost of health services [56], and the elevated costs of local providers [52]. One study [52] reported that the local provider was more expensive than travelling to a nearby town for the same service. Other studies reported cost barriers associated with emergency contraception and abortion services [39, 59]. The costs of essential sanitary products were also found to be high in rural areas, with local stores stocking low-quality options at expensive prices [54].
Demand barriers
Two barriers were found to hinder a woman’s ability to pay for healthcare: high travel-related costs and the financial burden of indirect costs. High travel-related costs were reported in four studies for women who were required to travel for care [40, 51, 56, 70]. Several studies identified the financial burden of indirect costs [15, 21, 39, 48, 59, 60]. Examples of indirect costs included transportation, accommodation, childcare, and loss of wages. Significant financial burdens were reported for women who needed to relocate for maternity care [46, 63]. For example, one study [46] reported the lack of financial support for partners who also relocated and incurred accommodation expenses while the mother was in the hospital.
Supply facilitators
Two facilitators emerged for affordability, including cost reduction strategies, and policy and incentive support. Cost reduction strategies involved the increased use of telehealth services due to lower associated costs [76]. Policy and incentive support included paid and subsidised local abortion service provisions to reduce travel [39], and nationally consistent pricing on sanitary products [54].
Demand facilitators
Service affordability was identified as a facilitator for women’s ability to pay for healthcare. Improving access and availability of MToP appointments and medication in rural areas was found to be much more affordable than accessing SToP [15]. Increased use of HPV self-sampling was another facilitator reported in studies, as this was often a no-cost service [65].
Appropriateness and ability to engage
Appropriateness refers to the overall clinical benefit for the woman and whether the expected health benefits (e.g., improved quality of life) outweigh the potential negative consequences (e.g., time, cost). Appropriateness also includes adequacy, which pertains to the quality of the type and model of services provided and their continuity [12]. The ability to engage relates to the woman’s participation in decision-making and treatment decisions, which is strongly influenced by the capacity to participate. The dimensions of appropriateness and ability to engage were explored in 28 studies across hospital (n = 13), primary care (n = 9), health promotion and prevention (n = 3), and specialist care (n = 3) settings.
Supply barriers
Two barriers were found for appropriateness: limitations in telehealth accessibility and care discontinuities. The limitations in telehealth accessibility were linked to language barriers for non-English speaking women and the absence of visual cues for the visually impaired [76]. Care discontinuities were documented in several studies relating to maternity care, particularly when women had to travel for care and had limited postnatal care options [45, 46, 69]. In one study, women reported concerns about care discontinuities in the context of assisted reproductive services due to facility shortages and restricted service provision [77].
Demand barriers
Two barriers were also identified for women’s ability to engage in healthcare, including a lack of support systems and psychological effects. Lack of support systems pertained to women who were required to relocate to give birth. Women who relocated experienced disconnection and distress from leaving family support and also reported inadequate caregiver support for existing children [63]. Another study reported that travelling to access abortion services meant leaving crucial support systems [59]. Insufficient childcare options to enable travel for care were also noted within lack of support systems [21]. Finally, the psychological effects stemming from access burdens and distress when trying to locate services was another identified barrier [59].
Supply facilitators
Two facilitators were identified for appropriateness, including telehealth accessibility and patient-centred care. One study found that the accessibility of telehealth helped to promote relationship-building with a provider before the patient was required to travel [76]. Patient-centred care, including continuity of care, was reported to be a facilitator in maternity care [53]. Knowing the woman’s story was particularly important in enhancing Aboriginal women’s experience with maternity care [53].
Quality appraisal
Thirty-nine studies (78%) were assessed using the JBI quality appraisal tool for qualitative design, while sixteen studies (32%) were evaluated using the JBI quality appraisal tool for analytical cross-sectional studies. A supplementary file includes the quality appraisal for all studies (see Supplementary file 3). All qualitative studies (n = 39) obtained ethical approval and adequately discussed the congruity between the research methodology, data collection methods, data analysis, and data interpretation. Most studies (n = 38) addressed the congruity between the research methodology and objectives. However, there were less common reporting on philosophical perspective (n = 15), locating the researcher culturally or theoretically (n = 9), and researcher reflexivity (n = 6). All cross-sectional studies (n = 16) adequately discussed the inclusion criteria, participants, settings, and outcome measures. Confounding variables were the lowest met criteria among studies, with majority of studies (n = 12) identifying them; however, only a small number (n = 2) stated strategies to deal with them.
This week’s Heads Up has the scoop on rental sports gear in the Outaouais, a farm-to-table dinner in Munster, a new bus to the Ottawa airport, a new restaurant in Kemptville, a bike ride near Eganville, açaí treats at St. Laurent Shopping Centre, day tripping to New Edinburgh and Rockcliffe, and more. Enjoy!
Cheese shop getting close to 100 percent Canadian stock
As you already know, I’m a big fan of supporting Canadian products—just check out my big guide to shopping locally. So a recent Facebook post by the Balderson Village Cheese Store, just outside Perth, caught my eye. The store’s owners have been making a concerted effort to stock 100 percent made-in-Canada foods. They’re about 75 percent of the way there and hope to have 100 percent Canadian stock by the end of the year. Well done!
You can rent scooters, pontoon boats and more in the Outaouais
Want to explore the great outdoors in the Outaouais, but you don’t have the gear? Tourisme Outaouais has this handy list of companies that rent out kayaks, paddleboards, canoes, electric bikes, scooters, pontoon boats and more.
OC Transpo to launch new bus to the airport
Perhaps finally realizing that folks travelling from Ottawa’s east end to Ottawa International Airport don’t much fancy taking three trains to reach their destination, OC Transpo is launching a direct bus service connecting the St. Laurent, Train and Hurdman stations to the airport. According to this CTV Ottawa story, Route 105 will launch on Sunday, August 24, and will run every half hour, 24 hours a day, seven days a week. The bus is anticipated to take 33 minutes to travel from St. Laurent to the airport.
Quebec loves its Nordic spas
Photo of Strøm Spa by Gaëlle Leroyer courtesy of Destination Québec Cité.
Quebec seems to have embraced the Nordic spa concept—the circuit of hot tub or sauna, cold pool or shower, relaxation and repeat—more strongly than just about anywhere else in Canada. I’ve written a post about some of my favourite Quebec Nordic spas, and it barely scratches the surface. My friend Hilary Nangle recently wrote a post about her favourite Quebec Nordic spas and while there’s a bit of overlap between the two pieces, she’s discovered quite a few spots that I haven’t made it to … yet.
Science fiction, fantasy and horror book convention is coming to Kanata
I wanted to mention this event on the website last year, but by the time I heard about it, it had sold out! So if you’re a fan of Canadian science fiction, fantasy and horror novels, you might want to get your ticket to Can*Con now. You can meet authors, buy books, take classes, pitch your own book to agents and more. It’s happening at the Brookstreet Hotel in Kanata from October 17 to 19.
New restaurant opens in Kemptville
Named for a famous local Holstein bull, Goldwyn’s restaurant opened this past weekend at 25 Clothier Street East in downtown Kemptville. It promises diners “a modern take on the Wild West at our elevated country western saloon.” Sounds like fun!
You can take a staycation in New Edinburgh and Rockcliffe
Fancy staying close to home? I have just the suggestion: a day spent exploring New Edinburgh, Lindenlea and Rockcliffe. From the new(ish) NCC River House on the Ottawa River to a posh grocery store and a great place to pick up consignment designer clothes, you can read my day trip tips in the Ottawa Business Journal.
Saunders Farm Pig and Corn Roast tickets are available
Most years, the farm-to-table Pig and Corn Roast at Saunders Farm in Munster sells out. So if you want to go to this year’s event on Sunday, August 24, you might want to get your tickets now.
Scenic August bike ride will take cyclists along Eganville backroads
If you want to challenge yourself to a self-supported, non-racing bike ride through the hills and along the backroads near Eganville, now’s the time to register for this year’s Tour de Bonnechere on Sunday, August 24. You can choose from 50km, 65km and 100km routes, as well as a 20km family ride.
You can try a superfood at St. Laurent Shopping Centre
Perhaps açaí berries are old hat to you. I’d heard of them but hadn’t had a chance to taste the Brazilian “superfood” until I was invited to try it at Rio Açaí at St. Laurent Shopping Centre. (The owners also have a location at 35 allée de Hambourg in Gatineau.)
Açaí berries have become trendy in recent years for their health benefits. At Rio Açaí, you can try them in a bowl with your choice of other fruits (I picked mangoes, strawberries and blueberries). The consistency of puréed açaí is a bit like tapioca pudding and it isn’t super sweet, so it made a nice combo with the sweet, dense fruit. You can also try other Brazilian specialties at the takeout spot, such as warm cheese bread (it’s really good) and, of course, coffee.
(Disclosure: I received free products for review purposes. The shop did not review or approve this post. All opinions are my own.)
As the owner of Ottawa Road Trips, I acknowledge that I live on, work in and travel through the unceded, unsurrendered territory of the Algonquin Anishinaabeg Nation. I am grateful to have the opportunity to be present on this land. Ottawa Road Trips supports Water First, a non-profit organization that helps address water challenges in Indigenous communities in Canada through education, training and meaningful collaboration.
Walk five minutes south of the monastery, past one former synagogue – Santa Maria La Blanca, reputed to be Europe’s oldest – and you arrive at another. The magnificent carved wooden ceilings and plasterwork walls of El Transito blend Mozarabic decorative influences. Constructed in 1355, El Transito houses the Sephardic Museum, which accounts for Toledo’s long Jewish history. You’ll find good information sheets in English and the museum has some especially beautiful ceramics. Pause afterwards in the synagogue’s small memorial garden. See spain.info
Take in the art at Hospital de Tavera
Patio in Hospital de Tavera museum.Credit: Alamy
Don’t like monuments and art? Better skip Toledo, which has them in spades. This Renaissance palace, built by a cardinal for the needy, is a whopper. The architectural highlight is the symmetrical double courtyards, while a wealth of paintings includes masterpieces by El Greco, Tintoretto and Zurbaran. Cardinal Tavera’s marble tomb is a sculptural work of art too, with no sign of humility other than a little memento mori skull tucked under his pillow. See fundacionmedinaceli.org
Admire El Greco paintings
Museum El Greco.Credit: iStock
Toledo is associated with El Greco, the 16th-century painter whose works seem astonishingly modern. You can see quite a few of his paintings in Toledo, and all are odd and electrifying. The church of Santo Domingo Monastery where the painter is buried has top examples including the altarpiece Assumption of the Virgin showing Mary springing from her tomb like a jack-in-the-box. El Greco Museum (in a house where El Greco never lived, despite claims) has several superb later works. See museodelgreco.sacatuentrada.es
Fill up at Confiteria Santo Tome
Santo Tome shop in Zocodover Square, Toledo.Credit: Alamy Stock Photo
If El Greco’s elongated, hollow-cheeked saints make you peckish, take a break from gloomy painted art and indulge in happy edible art instead. Toledo nuns are said to have invented marzipan – which is disputed – but Toledo has certainly produced it for centuries. Santo Tome, in business since 1856, is Spain’s best-known marzipan maker. You can devour biscuits, pastries, cakes, sweets and marzipan fruit filled with lip-licking goo. Like El Greco’s saints, you’ll soon be in heaven. See mazapan.com
Take a hike to Mirador del Valle
There are sweeping views of Toledo and the Tagus River from Mirador del Valle.Credit: iStock
Loading
In this old town of closed-in alleys, you’ll want to get beyond the walls to admire Toledo’s fabulous setting above the Tagus River, dominated by the whopping Alcazar, or fortress. This viewpoint is a 40-minute walk from Puente Nuevo bridge just below the fortress, but outlooks are fabulous all the way. Sunset and twilight are the most atmospheric. The lazy option is a taxi to nearby Parador de Toledo for a cocktail on the terrace. See paradores.es
Social media has a way of airbrushing reality, especially when it comes to travel.
Many people plan their entire vacations based on viral TikToks and Instagram photo ops, often without realizing what those places are actually like behind the lens.
I’ve been lucky enough to explore over 20 countries, and have been everywhere from the Arctic Circle and the European countryside to the Caribbean.
I love snapping photos and curating videos of my adventures along the way, but I’ll also admit that social media can make every trip look like a dreamy highlight reel with perfect sunsets, pristine hotel rooms, or bucket-list adventures.
Although I’ll always be grateful for the chance to see the world, the truth is, not every moment is as glamorous as it looks online.
Visiting Hollywood Boulevard isn’t as glitzy as it seems.
As a kid, I always glamorized the idea of visiting Hollywood.
Chloe Caldwell
As someone who grew up in the Los Angeles area, I’m incredibly familiar with every tourist hot spot in the city. As a product of the suburbs, I glamorized the idea of visiting Hollywood and immersing myself among those famous sidewalk stars.
The truth, though, is that Hollywood Boulevard is packed with crowds, speckled with trash, and has lots of overpriced attractions and gift shops.
If you want a good view of the Hollywood sign, I recommend going to Griffith Park Observatory instead. There, you’ll get an up-close look at the landmark and sweeping views of LA.
Taking a gondola ride in Venice can be expensive.
Taking a gondola ride in Venice is an incredible — but pricey — experience.
Chloe Caldwell
Venice has become one of my favorite cities for its dreamy waterways, cobblestone alleys, and vibrant atmosphere.
I’ve visited over the past two years and have plans to return this summer. Although a gondola ride might seem like a Venice rite of passage, I have a hard time justifying a nearly $100 price tag for a 30-minute ride.
It may be worth the splurge if a ride is a must on your itinerary. However, it’s also worth looking into the public gondola transfers (aka the traghetto) across the larger waterways that only cost 2 euros (about $2.35).
You’ll be with a group of people for a short, 3-minute ride, but you can still get a quick snapshot of yourself on the gondola.
Mānoa Falls in Honolulu can get crowded.
Mānoa Falls is a 150-foot waterfall near Honolulu.
Chloe Caldwell
The Mānoa Falls Trail is a lush, 1.6-mile round-trip hike near Honolulu that leads to a 150-foot-tall waterfall. It’s a gorgeous trail that I think is worth doing during your visit to Oahu.
However, in my experience, it’s not as serene as it seems online, and there will likely be crowds gathered at the waterfall’s base and the viewpoints throughout.
You’ll likely have difficulty getting photos without people in the background, especially if they’re swimming in the fall’s natural pool. I only got a decent picture of myself in front of the waterfall because it started raining and everyone else left.
I’d recommend going early in the morning to beat some of the rush, or going on a gloomy day when there might be fewer people on the trail. Also, keep an eye out for outlets along the way to find small and secluded streams.
The northern lights are much more vibrant in photos.
Photos of the northern lights often appear more vivid than the in-person display.
Chloe Caldwell
Don’t get me wrong: seeing the northern lights in Iceland was one of the best travel experiences of my life.
However, the photos you see online often make them look like a much more saturated version of what they actually look like to the naked eye. More often, the lights are a faint haze of subtle hues.
Although photos typically appear more vivid and colorful than the in-person display, watching the colors dance in the sky is awe-inspiring nonetheless.